

5-氟尿嘧啶封装 Ethosomes 联合 CO2 点阵激光治疗增生性瘢痕的实验研究
摘要
目标
本研究旨在探索由 CO2 点阵激光介导的 5-氟尿嘧啶 (5-FU) 包裹的 ethosomes 对肥厚性瘢痕组织的渗透性。此外,还将评估CO2点阵激光联合5-FU包裹的ethosome在兔耳肥厚性瘢痕模型中的治疗和持续时间效果。
方法
5-FU的渗透量和5-FU的保留量均采用高效液相色谱法(HPLC)测定。通过共聚焦激光扫描显微镜 (CLSM) 测量用 Rodanmin 6GO (Rho) 标记的 5-FU (5E) 封装的 Ethosomes 的荧光强度。在照射后 0 小时、6 小时、12 小时、24 小时、3 天和 7 天评估了用 Rho 标记的 5E 在 CO2 点阵激光介导的兔耳肥厚性瘢痕中的渗透性促进作用。根据 CLSM 计算微通道的打开率。在体内评价5EL对兔耳肥厚性瘢痕的治疗效果。用卡尺法测量治疗前后兔耳肥厚性瘢痕的相对厚度。 H&E染色测定兔耳增生性瘢痕瘢痕升高指数(SEI)。
结果
数据显示5EL组的渗透量高于5E组(4.15 ± 2.22 vs. 0.73 ± 0.33;p <0.05) 处理 1 小时后。此外,5EL的渗透量高于5E组(107.61 ± 13.27 vs. 20.73 ± 3.77;p <0.05) 处理 24 小时后。 5EL组的保留含量也高于5E组(24.42 ± 4.37 vs.12.25 ± 1.64;p <0.05)。在不同时间点(1、6和24小时),5EL组肥厚性瘢痕组织中Rho的荧光强度高于5E组。微通道的开放率在 24 小时内逐渐降低,微通道在 CO2 点阵激光照射后 3 天完全关闭。 5EL组治疗7天后兔耳肥厚性瘢痕相对厚度和SEI明显低于5E组。
结论
CO2点阵激光联合局部5E可有效治疗体内增生性瘢痕,为人类增生性瘢痕提供一种新的治疗方法。
背景
肥厚性瘢痕是一种皮肤病,其特征是胶原蛋白沉积过多,导致瘢痕隆起,但未达到观察到的瘢痕疙瘩[1]。由于5500万次择期手术和2500万次创伤后手术,发达国家每年共有1亿患者形成疤痕[2]。手术后,大约 60% 的患者在术后出现肥厚性疤痕,通常是在前 3 个月。大多数肥厚性疤痕在手术后 12 个月内仍是肥厚的 [3]。目前,常见的治疗方法包括手术治疗和非手术治疗。压力疗法、放射疗法、化学疗法和其他药物手术疗法是主要的疗法治疗。迄今为止,这些疗法由于存在缺陷而未能达到预期的治疗效果[4, 5]。药物治疗是基于局部注射的病理性瘢痕外涂治疗,是最常见的非手术治疗方法之一。由于药物副作用,局部注射往往仅限于小规模、低剂量的治疗。此外,由于药物半衰期短,局部注射药物在瘢痕处始终不能保持持久的高浓度;因此,经常需要重复注射 [6]。考虑到疤痕组织的密度和剧烈的疼痛,患者通常不接受注射。尽管具有无痛、对肝脏无副作用、便于长期外用等优点[7, 8],但由于病理性瘢痕组织结构特殊,药物无法进入瘢痕处。最近的报道还表明,局部用药很难穿透疤痕组织[9]。所以目前药物的外用是有限的。
Ethosomes 是 Touitou 在 2000 年使用的一种新型脂质载体 [10],可有效通过皮肤输送药物。乙醇脂质体的主要成分是乙醇,可以改变角质层脂质分子的紧密排列,增强脂质流动性,促进乙醇脂质体膜的弹性和流动性。来自乙醇酸的乙醇还可以加速角质层的变形,通过皮肤中紊乱的角质层增强其携带和渗透药物的能力[11,12,13]。然而,与正常皮肤组织不同,疤痕组织具有特殊的结构。在我们之前的研究中,我们证明了 ethosomes 是人类疤痕中药物的高效载体 [14]。疤痕组织中的药物分布不均匀,而是从皮肤外向内显着减少是必不可少的。药物主要积聚在表皮和真皮浅层,而不是真皮的所有层,从而降低抗瘢痕形成作用。
剥脱点阵激光治疗是一种美容技术,是目前非常流行和广泛接受的方式,主要用于临床治疗面部皱纹、浅表疤痕、色素沉着障碍和改善皮肤质地[15,16,17]。基于点阵光热解理论 [18],烧蚀点阵激光产生阵列状排列的微小激光束,并通过创建被热损伤区域包围的烧蚀微观垂直通道破坏皮肤屏障,诱导对中度皮肤的伤口愈合反应外观 [19,20,21,22]。据报道,药物经皮吸收的主要屏障是角质层 [23, 24]。近年研究表明,CO2点阵激光是临床最常用的点阵剥脱之一,能够击穿角质层,形成致密的微孔通道,从而破坏阻碍药物经皮吸收的主要屏障,具有良好的透皮促进药物渗透前景。 25,26,27,28]。
在这项研究中,我们在人类疤痕样本和兔耳肥厚性疤痕模型中探索了携带抗疤痕药物 5-氟尿嘧啶 (5-FU) 的 CO2 点阵激光介导的乙醇酸凝胶。使用这种新方法,我们专注于提高抗疤痕药物给药的效率,以缩短漫长的疤痕治疗过程。首次应用兔耳肥厚性瘢痕模型确定CO2分数激光介导的携带5-FU的纳米级脂质体对肥厚性瘢痕和药物渗透的影响。综上所述,CO2点阵激光联合局部药物治疗为人类增生性瘢痕提供了一种新的治疗方法。
方法
5-FU 封装 Ethosomes
Touitou 的方法 [10] 用于制备 5-FU 封装的 ethosomes。使用激光粒度分析仪 (λ) 确定 25°C 的粒度分布和多分散指数 (PDI) =632.8 纳米)。 PDI <0.1 表示粒径分布均匀,PDI> 0.3 表示粒径分布不均匀。透射电子显微镜 (TEM) 用于观察 Ethosome 的形态。本研究采用超速离心法[29]测定ethosomes的包封率(EE)。
高效液相色谱
Franz 细胞受体隔室中 5-FU 的浓度通过 Waters 2695 HPLC 系统(Meadows Instrumentation,伊利诺伊州)和 2487 紫外线检测器与反相 Diamonsil TM C18 柱(250 mm × 4.6 mm,5 μm)测定)。 5-FU 在 265 nm 处用甲醇-H2O (5:95 v /v ) 流速为 1 毫升/分钟。数据采用Waters Empower系统,通过峰面积和外标法进行分析。
共聚焦激光扫描显微镜
通过共聚焦激光扫描显微镜 (CLSM) 以 10 μm 的增量分析人类肥厚性瘢痕组织。使用带有 Fluar 10×、0.5 数值孔径物镜的激光扫描显微镜 LSM 510(Zeiss,Jena,Germany)分析荧光强度。用 543 nm HeNe 激光器进行光激发,并在 560 nm 以上检测到罗丹明 6GO (Rho) 的荧光发射。通过Release Version 4.0 SP2图像分析软件对图像进行分析,计算瘢痕组织的荧光分布和荧光强度。在10 × 10倍视场内,像素值的大小和分布确定5-FU EG(用Rho标记)的穿透范围,并采用半定量方法。
人类瘢痕组织中的 5-FU Ethosomes 渗透性测定
上海交通大学附属第九人民整形外科医院人增生性瘢痕标本取自瘢痕切除患者3例,均为女性,年龄21-35岁;疤痕位于肩部和背部; 6 个月至 1 年的增生性瘢痕病程;疤痕组织完整性;无溃疡;无感染病灶;而且最低的疤痕也必须高于皮肤,而且患者自患病以来没有接受过任何治疗。全身麻醉用于消除局麻药对瘢痕组织的影响。将所得标本立即从皮下组织中取出,保护表皮,制成厚度为4.0mm,面积为3cm × 3cm的瘢痕组织样品,室温下生理盐水冲洗,纱布擦干表面水分,包裹铝箔,并储存在 - 20 °C 的冰箱中。使用前,人类肥厚性疤痕组织被移除并储存在 - 20 °C 的冰箱中。将人肥厚性瘢痕组织在 25°C 下浸入 pH 7.4 PBS 2 小时,并用干纱布轻轻去除组织表面的水。增生性瘢痕组织的所有表皮组织区域均经CO2点阵激光照射。激光参数紧随其后的是 DeepFX 模式、25 mj 能量密度、20% 覆盖率、300 Hz 发射频率、10 号光斑尺寸且无重叠。所有辐照样品均采用高效液相色谱法检测,测定瘢痕组织中5-FU的含量。组织病理切片立即用于CLSM测定。
兔耳肥厚性瘢痕模型
兔耳肥厚性瘢痕模型制作方法简述如下:12只新西兰大白兔,雄性,体重2公斤(SLAC,上海),分别饲养2周。对于兔麻醉,通过肌内注射将鲁米宁与每 100 克体重 1.5 毫克氯胺酮混合。所有的伤口都被兔耳的中心点包围。每个直径 1 厘米的圆形伤口都有缺陷,然后去除软骨膜。术后二十八天,兔耳创面结痂,完全愈合,可见直径约0.9厘米的增生性瘢痕。疤痕呈鲜红色,明显增生周围皮肤有肿块,疤痕厚而硬。
微信开通率确定
兔耳增生性瘢痕模型CO2点阵激光治疗后不同时间点,红色荧光Rodanmin 6GO with ethosomes应用于瘢痕组织。三小时后,CLSM用于确定通道开放率。通道开放率=开放通道数/(开放通道数+封闭通道数)×100%。通道开放率的百分比反映了CO2点阵激光穿透效果的影响。
H&E 染色
通常,使用 10% 戊巴比妥 i.v. 处死兔子。注射(麻醉正常剂量的 5 倍,35 毫克/公斤)。立即取出标本并进行 H&E 染色步骤。苏木精伊红染色方法按标准H&E染色方案进行。
疤痕高度指数和相对厚度测定
兔耳增生性瘢痕诱导28天后,进行四组干预: 5EL组:5-FU包裹的内体凝胶联合CO2点阵激光; 5E组:5-FU包裹的内体凝胶; CO2组:CO2点阵激光治疗;和对照组。我们将A定义为兔耳增生性瘢痕组织最厚部分的厚度,B定义为距兔耳增生性瘢痕组织最厚部分(靠近中心点)1.0 cm处的厚度。相对厚度按A/B计算。 SEI 说明了真皮瘢痕肥大。 SEI =新形成的真皮面积/未受伤的真皮面积。 SEI> 1.5 表现为增生性瘢痕。
静态
所有实验均重复 3 次。数据表示为平均值 ± 标准偏差(SD)。使用 SPSS 19.0 版(SPSS Inc.,Chicago,USA)进行统计分析。学生的t 检验用于计算显着性。 *p 值 <0.05 被认为具有统计学意义; **p 值 <0.01 被认为在统计上非常显着; ***p 值 <0.001 被认为在统计上极其显着,并且 ****p 值 <0.0001 被认为在统计上非常显着。
结果
用 5-氟尿嘧啶 (5E) 封装的 Ethosomes 的质量评估
首先,为了验证用 5-氟尿嘧啶 (5E) 封装的 ethosomal 凝胶的质量,通过透射电子显微镜 (TEM) 观察检测形态和直径。悬浮状态的 Ethosomes 形成一个通用大小的完整圆形或椭圆球形囊泡,在显微镜下小于 100 nm(图 1a-b)。凝胶配制后,ethosomes 保持完整(图 1c-d)。使用激光粒度分析仪,悬浮状态的 Ethosome 直径似乎为 87.72 ± 9.27 nm,PDI 为 0.10 ± 0.01。同时,ethosomes的粒径为98.78 ± 10.88 nm,PDI为0.11 ± 0.02。静力学比较表明,粒径没有显着差异(p> 0.05)。此外,两个 PDI 没有显着差异 (p> 0.05)。此外,从激光粒度分析仪和 TEM 获得的数据显示了可比较的结果。此外,还使用超速离心法测定包封效率 (EE)(表 1)。结果表明,乙醇酸悬浮液的EE为10.47 ± 1.47%,乙醇酸凝胶的EE为11.56 ± 1.12%(n =6),没有显着性 (p> 0.05)。综上所述,Ethosome在悬浮状态和凝胶状态下均未发现形态和粒径变化。
<图片>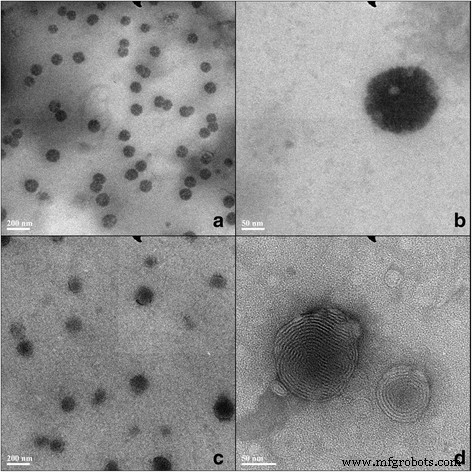
5-FU ethosome 的透射电子显微镜图像。溶液的 Ethosomes (a 和 b ) 和凝胶体 (c 和 d )
CO2 点阵激光通过体外增生性疤痕促进 5E 渗透
在评估了用 5-氟尿嘧啶 (5-FU) 封装的 ethosomes 的质量后,我们在体外使用或不使用 CO2 点阵激光研究了其在人类肥厚性瘢痕中的渗透性。 用CO2点阵激光照射人体增生性瘢痕组织,然后均匀涂抹5E。 5-FU 的累积浓度在 1、3、6、10、16 和 24 小时通过 HPLC 测定 (2)。我们比较了5-氟尿嘧啶(5EL)组和5E组在不同时间点与CO2点阵激光结合的5-FU累积浓度。 1 h时,5EL组的5-FU累积浓度为4.15 ± 2.22 μg/ml/cm 2 , 高于 5E 组的浓度 (0.73 ± 0.33 μg/ml/cm 2 , p <0.001)。在长期治疗(24 h)中,5EL组的5-FU累积渗透浓度(107.61 ± 13.27 μg/ml/cm 2 ) 也高于 5E 组 (20.73 ± 3.77 μg/ml/cm 2 , p <0.0001)。在较早的时间点,3、6、10 和 16 小时,5EL 组总是显示出比 5E 组更高的 5-FU 累积渗透浓度(图 2a)。此外,5EL组中5-FU的保留量为24.42 ± 4.37 μg/cm 2 , 高于 5E 组 (12.45 ± 1.64 μg/cm 2 , p <0.01, n =6)(图 2b)。该结果提示CO2点阵激光照射可显着促进脂质体中5-FU通过人增生性瘢痕组织,并有助于5-FU在体外增生性瘢痕组织中的滞留。
<图片>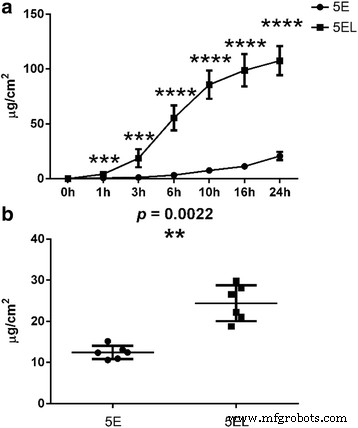
CO2点阵激光通过体外增生性瘢痕促进5E通透性。 一 5E和5EL组在体外人增生性瘢痕24小时研究中的渗透性比较。数值表示为平均值 ± SD。 n =6.b 应用 24 小时后,5-FU 在体外增生性瘢痕中的累积保留。 n =6.***p 值 <0.001 被认为具有统计学意义,****p 值 <0.0001 被认为在统计上非常显着
使用Rho标记的5E测定5-FU穿透的深度和程度,以评估CO2点阵激光在体外的增强穿透效果。荧光测定用于指示 5-FU 处理后 1、6 和 24 小时时 5E 和 5EL 组的强度(图 3a)。结果表明,5EL处理1h后,Rho荧光分布在表皮和真皮浅层,尤其是CO2点阵激光气化区周围。相比之下,在没有 CO2 点阵激光照射的情况下,Rho 荧光分布仅限于 5E 组的表皮区域。在 5EL 组处理 6 小时后,Rho 荧光扩展到真皮深层并表现出更多的积累。虽然5E组的荧光分布开始出现在真皮中,但荧光强度从真皮到表皮逐渐减弱。治疗24 h后,两组的荧光在整个皮肤组织中广泛分布,但5EL组的荧光强度明显更高。此外,Release Version 4.0 SP2 图像分析软件用于定量分析以计算两组的荧光强度。定量分析结果显示,5EL组的Rho荧光强度显着高于5E组(1h:59.61 ± 6.39 vs.6.39 ± 1.64,p <0.0001; 6 小时:163.32 ± 13.23 与 49.89 ± 4.01,p <0.0001; 24 小时:270.36 ± 8.73vs。 148.25 ± 16.89,p <0.0001)(图 3b)。综上所述,CO2点阵激光显着促进5E在体外对人增生性瘢痕组织的渗透。
<图片>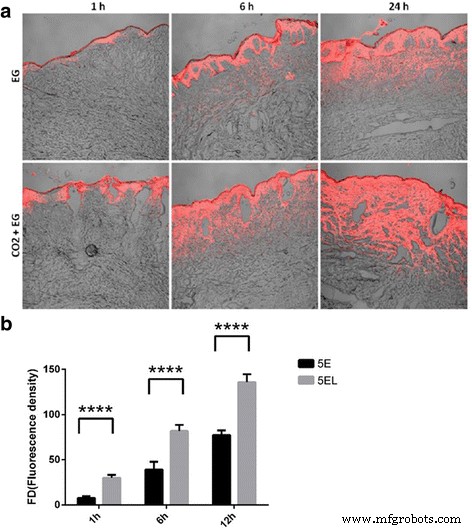
CO2 点阵激光通过体外增生性瘢痕促进渗透。 一 在体外 1、6 和 24 小时后,红色荧光标记为渗入肥厚瘢痕组织的 ethosome。 b 1、6 和 24 小时后,罗丹明 6GO 的荧光强度在体外标记肥厚性瘢痕组织上的 ethosome。 ****p 值 <0.0001 被认为在统计上非常显着
CO2 点阵激光的持续时间增强了体内 5-FU 的渗透
为了获得更多关于 CO2 点阵激光效应的证据,我们使用兔肥厚性瘢痕模型在体内进行了 5-FU 穿透。兔肥厚性瘢痕模型设置被描述为方法。在应用 CO2 点阵激光后的不同时间点(3 小时、6 小时、12 小时、24 小时、3 天和 7 天),进行 5E 或 5EL 处理,并通过 CLSM 立即确定荧光分布(图 4)。 Rho荧光广泛可见并广泛分布在兔耳肥厚性瘢痕的真皮层中,靠近烧蚀区(图4a)。这些结果可能表明,在 CO2 点阵激光照射后,与 5E 混合的 Rho 主要通过多孔通道渗透。 6 小时 5EL 后,即使分布区域很小,也可以在真皮组织周围的烧蚀区检测到荧光(图 4b)。荧光分布区域在药物处理后 12 小时继续缩小,这表明微孔通道在伤口愈合时逐渐关闭(图 4c)。经 CO2 点阵激光照射 24 h、3 天和 7 天后,荧光只能在开口周围的地壳孔隙内发现,没有渗透到真皮中(图 4d-f),这表明 CO2 点阵激光穿透效应随着表皮完全再上皮化而消失。我们的数据表明,微通道开放在 5EL 治疗的药物渗透中起着关键作用。此后,我们分别计算了激光照射后 3 小时、6 小时、12 小时、24 小时、3 天和 7 天的微通道打开率。在 3 小时和 6 小时的时间点,微孔通道全部打开,表明微通道打开率为 100%。微通道打开率在 12 小时开始下降到 90.59%,在 24 小时下降到 15.58%。特别是,微孔通道在 5EL 处理后第 3 天和第 7 天全部关闭。综上所述,这些结果表明CO2点阵激光在体内控制了兔肥厚性瘢痕组织中的药物渗透。
<图片>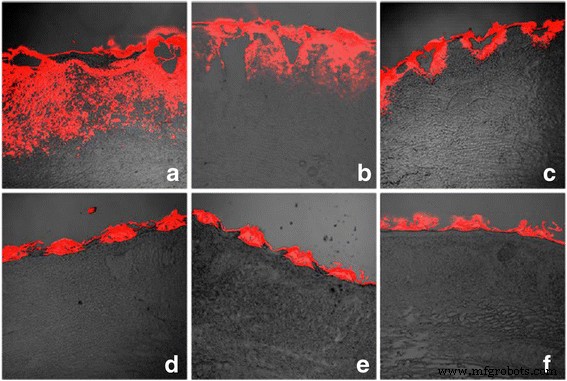
CO2 点阵激光促进体内微通道开放率。 0 h (a ), 6 h (b ), 12 小时 (c ), 24 小时 (d ), 3 天 (e ) 和 7 天 (f ) 体内 CO2 点阵激光治疗后
5EL对体内增生性瘢痕的治疗作用
为了深入了解5EL治疗,我们进行了兔耳增生性瘢痕相对厚度的测定。兔耳增生性瘢痕模型建立后,计算5EL治疗前后的相对厚度值。治疗前各组无显着差异。而5EL组的相对厚度为1.27 ± 0.15,明显低于5E组(1.52 ± 0.10,p <0.05) 和未处理 (1.61 ± 0.15, p <0.0001) 组(图 5)。有趣的是,仅 CO2 激光治疗组和 5EL 组之间没有显着变化。这些数据表明CO2点阵激光在体内治疗兔耳肥厚性瘢痕中起主导作用。
<图片>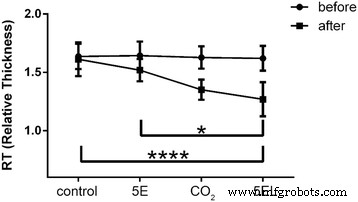
不同治疗前后兔肥厚性瘢痕相对厚度的比较。 5EL:5-FU包封的内体凝胶结合CO2点阵激光,n =14; CO2:仅 CO2 点阵激光,n =12; 5E组:5-FU包裹的内体凝胶,n =14;控制:空白,n =16.*p 值 <0.001 被认为是显着的,****p 值 <0.0001 被认为在统计上非常显着
我们还比较了兔耳肥厚性瘢痕的形态,以确定使用 CO2 点阵激光的差异。在 5EL 组中,增生性疤痕变平,颜色明显变为淡粉色(图 6a-b)。在仅 CO2 点阵激光治疗组中,增生性瘢痕厚度有所减少,其颜色变为淡红色(图 6c-d)。在 5E 组中,增生性瘢痕厚度略有减少,但颜色保持鲜红色(图 6e-f)。最后,与治疗前相比,未治疗组没有显着变化(图 6g-h)。接下来,对这四组兔耳肥厚性瘢痕组织在治疗后7天使用H&E染色进行病理分析(图7)。 5EL 组和仅 CO2 点阵激光治疗组显示增生性瘢痕和点状痂皮层厚度减少,真皮浅层胶原纤维少见结节状或螺旋状排列(图 7a-b)。在5E组和未处理组中发现大量真皮胶原纤维渗透,胶原纤维排列紊乱,以及表层真皮结节状或螺旋状排列(图7c-d)。增生性瘢痕的另一个重要评估方法是瘢痕升高指数(SEI)。与相对厚度模式相似,与5E组(1.32 ± 0.13)和未治疗组(1.49 ± 0.13)相比,5EL组(1.16 ± 0.08)和仅CO2点阵激光治疗组(1.22 ± 0.10)的SEI显着降低(1.49 ± 0.10) . 8)综上所述,形态学分析和SEI计算数据表明CO2点阵激光在体内愈合兔耳肥厚性瘢痕的作用。
<图片>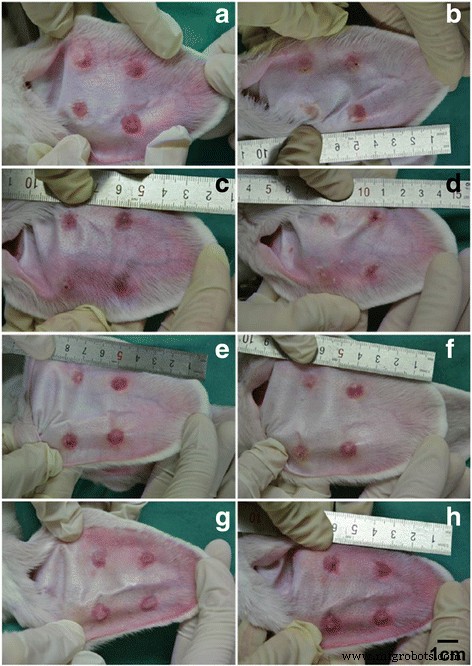
兔肥厚性瘢痕在应用不同治疗 7 天前后的照片成像。 5EL组:5-FU包封的内体凝胶结合CO2点阵激光,在(a ) 和之后 (b ) 治疗 7 天; CO2组:CO2点阵激光,之前(c ) 和之后 (d ) 治疗 7 天; 5E B 组:用 5-FU 包封的内体凝胶,之前 (e ) 和之后 (f ) 治疗 7 天;和空白组:空白,之前 (g ) 和之后 (h ) 治疗 7 天
<图片>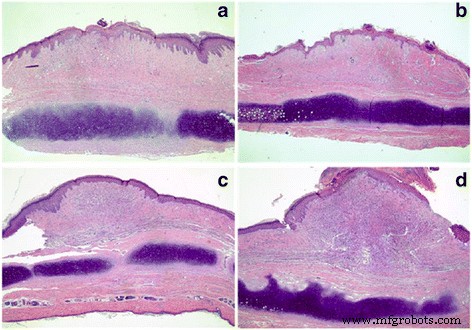
应用不同治疗 7 天后兔肥厚性瘢痕的 H&E 组织学分析。 5EL组:5-FU包裹的内体凝胶结合CO2点阵激光(a ); CO2 组:CO2 点阵激光治疗 (b ); 5E组:包封5-FU(c );和空白组:空白 (d )。原始放大倍数:× 40
<图片>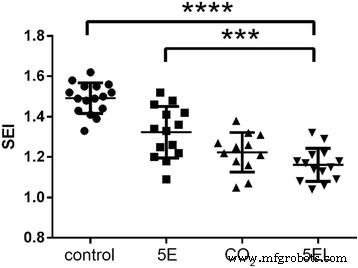
兔肥厚性瘢痕在应用不同治疗 7 天后的 SEI 比较。 5EL:5-FU包封的内体凝胶结合CO2点阵激光,n =14; CO2:CO2点阵激光,n =12; 5E:用 5-FU 包裹的内体凝胶,n =14;控制:空白,n =16.***p 值 <0.001 被认为在统计上极其显着,****p 值 <0.0001 被认为在统计上非常显着
讨论
药物治疗是主要的治疗方法,主要是外用或局部注射,用于增生性瘢痕的非手术治疗。由于各种药物的副作用,局部注射往往限于小剂量,因此只能进行小范围的治疗。此外,由于药物的半衰期短,疤痕中持续的高浓度需要重复注射 [6, 30, 31]。此外,由于瘢痕组织非常集中,注射时常有剧烈疼痛,患者往往不愿接受治疗。外用药虽然具有方便、无痛、长期稳定、副作用小、不受胃肠环境影响等优点[7, 8],但也存在一些局限性。首先,局部和注射药物的可用性受到特殊病理瘢痕组织结构的限制,表现为角质层增厚和真皮增生,阻碍了药物的渗透和达到有效治疗浓度。 Recent reports have proven this and described how external use of drugs inefficiently penetrates the scar tissue [4, 9]. Ethosomes, proposed by Touitou et al. [10] in 2000 as a transdermal drug carrier, have been widely reported [11, 12, 32]. In this study, we improved the ethosomes preparation process to nano-level (particle size 70~90 nm). This change of a new nanoscale dimensions and the spatial conformation of the ethosomes allow them to penetrate into the scar tissue through a narrowly tightly connected cell gap not only due to the small size, but also by the similarity to the cell membrane of scar tissue cells. Based on such penetration mechanisms, ethosomes become a convenient transdermal drug carrier [14, 33, 34]. However, the anti-scar drug 5-FU encapsulated with ethosomes is mainly concentrated in the epidermis and dermis, which is not conducive to fibroblasts in deeper layers of the dermis. Therefore, our purpose is to explore a method that would allow to increase the penetration of drugs and would promote the uniform dispersion of drugs in scar tissue.
So far, commonly used methods to promote the penetration are divided into two categories:the promotion of chemical substances and physical methods to enhance permeability. The physical enhancement techniques include electroporation, iontophoresis, laser, microdermabrasion, microneedle, pressure, radiofrequency induction, and sonography [35]. There are many different types of lasers that have been shown to promote percutaneous administration, and ablative fractional lasers become the most popular laser in recent years for promoting drug penetration into the skin [20]. Ablative fractional laser can not only extremely reduce drug dosage, but also be conducive to drug penetration into deep skin and achieve high local concentrations to obtain a therapeutic effect. CO2 fractional laser, Erbium-doped Yttrium Aluminum Garnet (Er:YAG) fractional laser, and Erbium-doped Yttrium Scandiu Gallium Garnet (Er:YSGG) fractional laser can produce ablative zone or microporous channels on the surface of the skin. Compared with Er:YAG fractional laser (2940 nm wavelength) and Er:YSGG fractional laser (2790 nm wavelength), CO2 fractional laser (10,600 nm wavelength) has lower water absorption coefficient, larger thermal damage, and greater destruction effect of stratum corneum of the epidermis, which is more conducive to promote penetration effect [36].
In this study, 5-FU retention in the 5EL group (24.42 ± 4.37 μg / cm 2 ) was significantly higher than in the 5E group (12.45 ± 1.64 μg/cm 2 ) in scar tissue of 24 h treatment in vitro. Additionally, in Rho-labeled assay, 5EL group has shown higher fluorescence intensity than 5E group at 1-, 6-, and 24-h treatment time points. Image analysis showed that fluorescence can be found distributed in the gasification zone and surrounding dermal tissue matrix after 1-h CO2 laser treatment in the 5EL group, and the fluorescence in 5E group is only distributed in the epidermis. After 6- and 24-h treatment, diffuse fluorescence range is wider and fluorescence intensity is higher in the 5EL group than in the 5E group. CO2 fractional laser-induced gasification zone provided an effective way for drug penetration through the skin scar tissue, enlarge range of dermis penetration depth, and retention content in scar tissue. There are three different forms of thermal effect damage by CO2 fractional laser acting on the skin or scar tissue, from center to outliner, the gasification zone, thermal coagulation necrosis zone, and thermal denaturation zone [37]. Fluorescence data showed that Rho fluorescence was distributed from more concentrated gasification zone to diffused tissue, suggesting that there is no effect for permeation of drugs in thermal coagulation necrosis zone and thermal denaturation zone, which also confirmed the feasibility of CO2 fractional laser for the promotion of topical anti-scarring drug penetration. Together, CO2 fractional laser is conducive to more anti-scarring drugs 5-FU retention in scar tissue and achieve high drug concentration required to strengthen the anti-scarring effect.
The duration of CO2 fractional laser enhancing 5E was evaluated by CLSM on rabbit ear hypertrophic scar in vivo. The opening rates of microporous channels for drug permeation were 100% (0 h), 100% (6 h), 90.59% (12 h), and decreased to 15.58% (24 h) after CO2 fractional laser treatment of hypertrophic scar. Moreover, microporous channel opening rates dropped to zero on 3 and 7 days, and the drug can no longer penetrate into the skin through these channels. These results were consistent with that of epidermal re-epithelialization after ablative fractional laser irradiation, which is the skin wound around the keratinocytes to the wound defect migration and proliferation, covering the wound to form a complete layer of cells formed by the epidermis. When the dermal layer of skin was wound, the repair process will immediately start and quickly rebuild the skin barrier [38, 39]. The whole skin tissue trauma repair process can be divided into four continuous and overlapping steps:coagulation, inflammation, re-epithelialization, and remodeling [40]. Human skin after ablation of the fractional laser irradiation injury area (including the gasification area and coagulation necrosis area) complete epidermal re-epithelialization in 2 to 3 days and dermal remodeling for at least 4 weeks [41]. Thus, although the lesion in the dermis does not heal within 24 h after the CO2 laser treatment, the epidermis has completed the complex epithelization, including the formation of the stratum corneum, where the topical drug could not penetrate through channels. Taken together, epidermis, especially the stratum corneum, is still the main barrier for drug penetration through the skin.
In addition, our CLSM data showed both in in vitro human hypertrophic scar skin and in vivo rabbit ear hypertrophic scar skin, Rho-labeled 5E can penetrate the necrotic coagulation layer and the formation of crust on the surface after the CO2 fractional laser irradiation. It suggested that the skin under the crust but not the coagulation necrotic layer and crust tissue can impede the penetration of drug. Therefore, 24 h is the critical time-point for the effect of CO2 fractional laser on the penetration effect of hypertrophic scar in rabbits.
It has been reported that the clinical application of exfoliative fractional laser is an effective method to treat various skin diseases (such as solar keratosis, basal cell carcinoma, Bowen’s disease, etc.) [25,26,27,28]. However, the clinical efficacy of CO2 fractional laser in combination with drugs has not been explored in the treatment of hypertrophic scars [42, 43]; in particular, there are no reports of combined CO2 fractional laser (physical technique) with anti-scar drug nano-level ethosomes (chemical substances promoting scar penetration) for the treatment of hypertrophic scars. Using in vivo study, we performed a rabbit hypertrophic scar model for validation of CO2 fractional laser protocol. On the seventh day after intervention, the relative thickness of the four groups of hypertrophic scar was measured:experimental group (CO2 fractional laser combined with 5-FU EG):1.27 ± 0.15
The toxicity of the ethosomes should be a big concern in this study. Nevertheless, after reviewing literature, there are no results exhibiting the toxicity of ethosomes in vitro or in vivo study [44,45,46]. The permeability mechanism of ethosomes is mainly as follows:high concentration of ethosomes, the flexibility, and fluidity of ethanol liposome membrane, makes ethosomes deform in the process of transmission, and enhances the permeability in scar tissue [47].
Although the difference between the experiment group and control group A was not statistically significant, the relative thickness and SEI of the experimental group was smaller than that in the control group A. Both groups were treated with CO2 fractional laser, with or without 5E. This finding suggests that CO2 fractional laser may have the dominant role, which overtakes the minor effect of 5E drug in the final anti-scar effect.
Conclusion
CO2 fractional laser can rapidly and significantly promote 5-fluorouracil encapsulated ethosomes’ permeability through hypertrophic scars in vitro. CO2 fractional laser is a potentially efficient method of promoting drug permeation in hypertrophic scars’ treatment. Our hypertrophic scar model (rabbit) showed that CO2 fractional laser combined with external-loaded 5-fluorouracil encapsulated ethosomes can effectively cure hypertrophic scars. Also, CO2 fractional laser itself can facilitate collagen remodeling in hypertrophic scar of rabbit ears. CO2 fractional laser can significantly promote the permeation of 5-fluorouracil encapsulated ethosomes, but the effect begins to relinquish 24 h after CO2 fractional laser irradiation, which indicates that 24 h is a critical period.
纳米材料